
COVID-19 Vaccination, Flu Vaccine and Pregnancy
COVID-19 Vaccination
The Pfizer-BioNTech COVID-19 vaccine is a new type of vaccine that has been shown to be effective and to have a good safety profile. It has not yet been assessed in pregnancy so it has been advised that until more information is available, those who are pregnant should not take this vaccine.Flu Vaccination
All pregnant women are encouraged to book an appointment with their GP or local pharmacy to access the free flu jab as soon as possible. The flu jab is one of the most effective ways to protect yourself this winter. Public Health England research has highlighted that if you get both COVID-19 and flu at the same time, you are much more likely to be seriously ill than if you are infected with one virus alone. Read this link for further information about the COVID-19 vaccine:Deep vein thrombosis in pregnancy

Deep vein thrombosis in pregnancy
 Being pregnant increases your risk of developing deep vein thrombosis (DVT), with the highest risk being after you have had your baby. However, a DVT can occur at any time during your pregnancy, including the first three months of pregnancy.
Being pregnant increases your risk of developing deep vein thrombosis (DVT), with the highest risk being after you have had your baby. However, a DVT can occur at any time during your pregnancy, including the first three months of pregnancy.
Signs/symptoms
- Pain/tenderness in the leg behind the knee or in the calf.
- Feeling of heat in the affected area or a red discolouration of the skin.
- Swelling of the affected area.
- A pulmonary embolism may cause shortness of breath and chest pain, which comes on suddenly and worsens with deep breaths, coughing or chest movement.
Treatment
These conditions are serious and will require urgent treatment in hospital with medications that prevent the clot from getting bigger and breaking off and travelling to another part of the body.Prevention
- Keep mobile and rotate your ankles regularly.
- Wear compression stockings if your midwife or doctor have advised you to do so.
- Consider taking short walks when you feel up to it.
- Stay well hydrated.
- Avoid sitting/lying down for prolonged periods, ie, in a car/on a train.
Listeriosis

Listeriosis
Altough rare, listeriosis infection in pregnancy can lead to miscarriage, stillbirth or severe illness in newborn babies. Listeria can be found in unpasteurised milk and in many chilled foods including pâté.
Commonly used medicines during pregnancy

Commonly used medicines during pregnancy
1. Analgesics (pain killers)
a) Paracetamol (500mg tablets)
What is it used for? Paracetamol is a commonly used pain killer in pregnancy. Paracetamol works by relieving pain and lowering high temperature. It can provide effective relief from mild to moderate pain, including headache, toothache, sore throat, symptomatic relief of rheumatic aches and pains, influenza symptoms and fever. How do I take it? Paracetamol can be taken regularly or when required for pain. Dosage: Adults and young persons aged 12 and over: take 2 tablets up to 4 times per day, as required. The tablets should be taken with water. Take only as much as you need to relieve symptom and leave at least 4 hours between each dose. Do not take more than 8 tablets in 23 hours. What are the side effects? Paracetamol is generally well-tolerated in most people. Is it safe to use during pregnancy? Paracetamol is commonly used during pregnancy.b) Co-dydramol
What is it used for? Co-dydramol (10/500 10mg dihydrocodeine and 500mg paracetamol) is a combination of paracetamol and dihydrocodeine. Dihydrocodeine is stronger than paracetamol and is used for the relief of mild to moderate pain. How do I take it? Dosage: Co-dydramol 1 to 2 tablets every 6 hours when required up to a maximum of 4 times per day. Do not take more than 8 tablets in 24 hours. We recommend that you step down pain relief and substitute these tablets for paracetamol as soon as possible which is usually after 3-4 days. Since these tablets contain paracetamol you should not take any other paracetamol tablets at the same time. Do not drink alcohol whilst taking co-dydramol. What are the side effects? The most common side effects of dihydrocodeine are drowsiness, constipation, feeling sick or dry mouth. You may be advised to take a gentle laxative if you experience constipation whilst taking co-dydramol. Is it safe to use during pregnancy? Use of dihydrocodeine during pregnancy as a pain killer can be justified where paracetamol has not been effective. Use the minimum effective does for the least amount of time. If you would like any further information regarding the use of dihydrocodeine in pregnancy, please discuss it with your midwife/doctor.2. Ferrous Sulphate (Iron supplements)
What is it used for? Iron supplements are used to treat iron deficiency anaemia. When the body does not get enough iron, it cannot produce the number of normal red blood cells needed to keep you in good health. It is common for women who are pregnant or who have just given birth to have this condition. These medicines work by replacing body iron. Iron is a mineral that the body needs to produce red blood cells. How should I take it? Swallow the tablets who with water. Although iron preparations are best absorbed on an empty stomach, they may be taken after food to reduce the effects on the stomach. Iron supplements should not be taken within one hour before or two hours after eating or drinking the following products: tea, coffee, milk, eggs and wholegrains. These products can reduce the absorption of iron. Dosage: Ferrous sulphate 200 mg tablets Treatment of iron deficiency anaemia: 1 tablet 2-3 times a day Prevention of iron deficiency anaemia: 1 tablet per day What are the side effects? Like all medicines, ferrous sulphate tablets may cause side effects, the most common of which are constipation, diarrhoea, stomach pain, feeling sick and blackened stools (faeces). Is it safe to use during pregnancy? Ferrous sulphate tablets are commonly used safely in pregnancy. Ensure that you do not take more than the recommended dose. If you cannot tolerate ferrous sulphate tablets, an alternative is available called ferrous fumarate. This is available as a liquid or tablets. The same side effect and safety information applies as above for ferrous sulphate.3. Laxatives
What are they used for? Laxatives are used to treat constipation. Pregnant women may experience constipation, which can be very uncomfortable. This is because the whole digestive system is influenced by hormonal changes during pregnancy. It is important for pregnancy women to look after their diet and maintain regular bowel habits to avoid unnecessary discomfort. What else can I do to prevent becoming constipated? The following hints are helpful in maintaining regular bowel habits:- Eat fibre-containing foods, e.g. wholegrain bread, fruit and vegetables.
- Drink sufficient liquid, preferably water.
- Take regular exercise.
a) Lactulose
Lactulose is a liquid laxative used to treat and prevent constipation. Lactulose can take 2-3 days to have an effect; it is generally considered to be a gentle laxative. Dosage: Usually 10 mls twice daily. It must be taken regularly to have an effect.b) Fybogel (Ispaghula husk)
Fybogel is a high fibre drink that works to increase the fibre in your diet. Increased fibre in the diet helps to gently relieve constipation. Fybogel is considered to be a gentle laxative. It is important to maintain an adequate intake of fluid whilst using Fybogel. Dosage: The usual dose is one sachet mixed with a glass of water, up to twice daily. Is it safe to use Lactulose or Fybogel during pregnancy? Lactulose and Fybogel are not absorbed into the blood and only have a local effect on the gut. Both drugs are generally considered safe to use in pregnancy and for breastfeeding, under the advice of a midwife or doctor.4. Blood clot prevention
Enoxaparin (also known as Clexane) is used to prevent blood clots. Blood clots usually present as deep vein thrombosis (DVT) usually in a leg vein, or pulmonary embolism (PE), a blood clot in the lung. Blood clots are more common during pregnancy and some women will be more at risk of blood clots than others. Your risk factors for developing a blood clot will be assessed at your booking appointment and if you are admitted to the hospital. As well as prevention, enoxaparin is also used at higher doses for treatment of DVT and PE. How is enoxaparin used during pregnancy? During the antenatal period, your midwife or obstetrician will assess your risk of developing a DVT/PE. They will look at your previous history and other risk factors that may exist. Your obstetrician will then decide if you require enoxaparin during pregnancy, and the dose you are to have. Is it safe to use during pregnancy? Enoxaparin is given as an injection just beneath the skin (subcutaneous). It is usually injected into a skin fold in your abdomen (stomach) or the upper part of your thigh. If this is not suitable, you may be advised to inject into an alternative site. It should not be injected into your muscles. It may be given either once or twice daily. You should administer the dose at the time recommended by your doctor. How to inject Enoxaparin (Clexane) You will be able to inject enoxaparin once you have been shown how to do so by your doctor or midwife, or by following the instruction leaflet that will be given to you upon discharge. It is a simple process and one that you can do at home. Follow these steps:- Wash and dry your hands.
- Clean the injection site. If someone else is doing it for you it is advisable that they wear gloves.
- Choose the injection site either on the outer aspect of your left or right thigh or your stomach if advised to do so. It is important that you change the site each time. If there is any oozing of blood at the injection site, apply gentle pressure. Do not rub as this may cause bruising.
- Dispose of the syringe in the yellow sharps box provided. This box should be kept out of the reach of other people.
Spontaneous Coronary Artery Dissection (SCAD) in pregnancy

Spontaneous Coronary Artery Dissection (SCAD) in pregnancy
SCAD is a rare but serious heart condition that causes a tear or bruise to develop in a coronary (heart) artery resulting in a blockage that prevents normal blood flow. It can cause heart attack, heart failure or cardiac arrest and can be fatal.
SCAD can happen during pregnancy and during the weeks and months after you have given birth. Symptoms can include:
- central chest pain
- arm pain or numbness
- pain in the jaw, back or shoulders
- nausea
- sweating/clamminess
- breathing difficulties
Preventing and managing common complaints during pregnancy

Preventing and managing common complaints during pregnancy
What complaints are common during pregnancy?
Pregnant women may experience one or more of the following symptoms:- back, pelvic, buttock or hip pain
- rib pain
- leakage of urine when coughing or sneezing
- aching legs/cramps/varicose veins/swollen ankles
- numbness and tingling in the hands
- fatigue (extreme tireness)
Why am I more likely to experience these common complaints during pregnancy?
Hormonal changes
From early on in your pregnancy your body produces high levels of certain pregnancy hormones (called ‘relaxin’ and ‘progesterone’). These work to soften ligaments and muscles, especially around your lower back and pelvis, preparing your body for pregnancy and labour.Weight gain and postural changes
Your body adjusts to the weight gain during pregnancy by changing your posture, for example, the way you stand. This can result in increased strain through some areas of your body. Strain is often felt around your lower back or pelvis.Muscular changes
Your abdominal (tummy) muscles act like a corset to support your spine. During pregnancy, they soften and stretch slightly to allow your baby to grow. This can make them less effective in supporting your back and pelvis. Other muscles may also stretch or weaken during pregnancy, including your pelvic floor muscles which help to control your bladder and bowels. All of these changes are normal and allow your body to adapt to being pregnant, but they can make you vulnerable to aches and pains. The advice on the following pages will help you to be aware of the changes occuring and how to take care of yourself during pregnancy.What can I do to help prevent aches and pains?
Look after your back
Think about your posture Doing this throughout your pregnancy can help to avoid and reduce pain.1. When you are standing:
Try to avoid your ‘bump’ pulling you forward and over-exaggerating the curve in your lower back:- Tuck your chin in
- Pull your shoulders back and down
- Gently draw your tummy button towards your spine
- Squeeze your buttocks slightly
- Keep your knees relaxed and soft
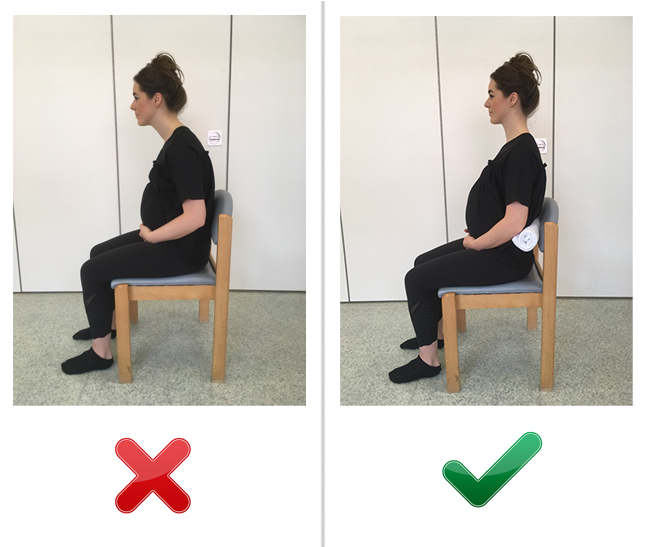
2. When you are sitting:
- Try not to slouch
- choose a chair that will provide your back with some support and ensure your bottom rests at the back of the chair. You may also wish to place a pillow or rolled up towel in the small of your back.
- Make sure your feet are flat on the floor
- try using a foot rest if they don’t quite reach. This will take the pressure off your spine.
- As you stand up from a chair or bed, try squeezing your tummy and buttock muscles to provide extra support to your pelvis.
3. When you are lying down:

- Lie on your side with a pillow between your knees (bending your knees comfortably).
- You may find a pillow or small towel placed under your ‘bump’ supportive.
- When turning from side to side, keep your kneeds bent and together, squeezing tummy and buttock muscle and moving in stages. Alternatively, turn onto all fours, keeping your buttocks clenched as you turn.
4. Geting in/out of bed
- Bend your hips and knees together and remain on your side.
- Squeeze your buttock and tummy muscles as you move.
- Push up with your arms into a sitting position.
- Do the reverse to get into bed or try climbing into bed on all fours.

5. What about lifting?
- Where possible, cut down on activities that involve bending, twisting and lifting, such as picking up small children and vacuuming
- When lifting from the floor, bend down on one knee – see picture opposite
- Keep a small stool to use in the kitchen to sit on instead of squatting down
- Avoid lifting excess weight where possible – your body is already working hard to carry your baby
- Shopping – try to avoid lifting out of deep shopping trolleys. When carrying larger loads, try to distribute the weight equally in each hand, or use a small backpack.

Tips for daily life
- Footwear
- avoid heels more than 1 inch in height and try to have flat shoes with a supportive arch as they can encourage good posture.
- Dressing
- sit down to get dressed. This avoids standing on one leg, which can aggravate pain.
- Ironing
- make sure the board is a waist level to avoid prolonged stooping. Alternatively, sit down to iron if possible.
- Cooking
- sit rather than stand when preparing food.
- Getting into a car
- sit down first, keep your knees togeher and then swing both legs in at the same time (or slowly move each leg). Reverse this to get out of a car.
Keep your tummy muscles strong
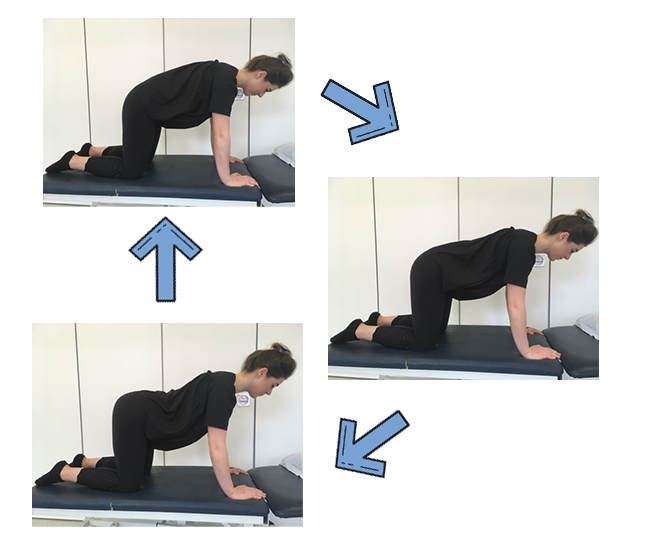
Your tummy muscles stretch during pregnancy to allow your baby to grow and this is normal. The following simple exercises are safe to do during pregnancy and can help relieve back pain and improve the strength and function of your lower tummer muscles. If you are unsure about any of the exercises, please speak to a physiotherapist before starting them.Transversus abdominus (deep lower tummy muscle)
This muscle wraps around your lower tummy and back like a corset to support the area. To strengthen this muscle:- Begin on your hands and knees (all fours), keeping your shoulders over your hands and your hips over your kneeds – try to keep your back flat and still.
- Breathe in, and as you breathe out, gently draw in your lower abdomen/tummy towards your spine.
- Hold for 10 seconds, then release.
- Repeat at least 10 times until fatigued.
- Try to practice this two or three times a day.
Pelvic tilting
- Stand with your back against a wall, with your head, shoulders and bottom touching the wall.
- Bend your knees, keeping your heels shoulder-width apart, feet slightly sway from the wall.
- Pull your tummy button back towards your spine and tuck your bottom under until you feel your lower back flatten against the wall.
- Repeat up to ten times and do the whole exercise three times a day.
 Alternatively, you can try doing this exercise in different positions, such as when kneeling, leaning on the bed, sitting (on a chair or exercise ball), or on all fours) see pictures 1-2 and a-c).
Alternatively, you can try doing this exercise in different positions, such as when kneeling, leaning on the bed, sitting (on a chair or exercise ball), or on all fours) see pictures 1-2 and a-c).
Keep your pelvic floor muscles strong
Your pelvic floor muscles lie between your public bone at the front and your coccyx (tailbone) at the back of your pelvis. They surround your anus, vagina and bladder openings. These muscles are like a platform that helps the pelvis to support the weight of your baby as it grows. They also maintain control of your bladder and bowels, and give support to the pelvic bones. During pregnancy, these muscles can be weakened by the weight of the baby, and are stretched during vaginal birth.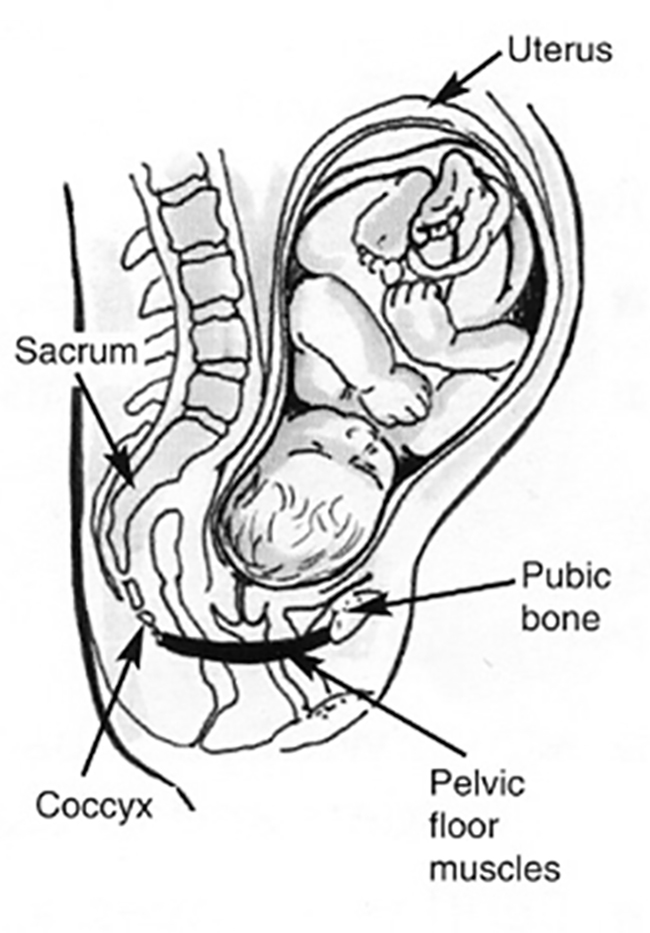 Some women may experience leakage of urine when coughing and sneezing (known as ‘stress urinary inconinence’) as a result of weak pelvic floor muscles. This is a common complaint affecting one in three women, but it can be prevented, reduced and even resolved fully with regular pelvic floor exercises.
It is highly recommended that all pregnant and postnatal women regularly exercise their pelvic floor muscles even if they have no problems with bladder control, to prevent problems in the future.
To begin with, you may have to concentrate while doing the exercises, but as you become more confident, you could do them whilst watching television, standing in a supermarket queue or waiting for the kettle to boil.
Some women may experience leakage of urine when coughing and sneezing (known as ‘stress urinary inconinence’) as a result of weak pelvic floor muscles. This is a common complaint affecting one in three women, but it can be prevented, reduced and even resolved fully with regular pelvic floor exercises.
It is highly recommended that all pregnant and postnatal women regularly exercise their pelvic floor muscles even if they have no problems with bladder control, to prevent problems in the future.
To begin with, you may have to concentrate while doing the exercises, but as you become more confident, you could do them whilst watching television, standing in a supermarket queue or waiting for the kettle to boil.
Pelvic floor exercises
Imagine you are trying to stop yourself passing wind and then pull forward as though you are also trying to stop your flow of urine. This closes and draws up the back passage and vagina. You need to exercise this muscle in two ways:1. Slow holds
Hold the muscle in for as long as you can for up to 10 seconds. Release slowly and rest for at least 5 seconds between each one. Aim to do 10 in a row.2. Fast squeezes
Squeeze the same muscles but quickly, releasing straight away. Aim to do 10 in a row. You can do these exercises almost anywhere and anytime but not when passing urine. In the beginning you will find these exercises easier to do when lying down or sitting. To train these muscles during and after pregnancy, try to get into the habit of doing both of the exercises 3-6 times a day.Other helpful tips
- If you have swollen ankles or legs, make sure you spend some time with your feet up every day. Keep your feet moving and avoid crossing your legs. Wearing support stockings may help.
- Sometimes women experience numbness and tingling in their hands. This can be due to excess fluid retention and often worse at night and first thing in the morning.
- Try running cold water over your hands for a few minutes when you wake up – this helps improve circulation. Keep your hands moving, and massage your hands in the direction of your elbows. If this remains a problem, ask your midwife or GP to refer you to a physiotherapist.
- It is hard work being pregnant, so listen to your body and rest when you need to. It is a good idea to spend some time relaxing regularly.
What about lower back and pelvic pain during pregnancy?
Lower back and pelvic pain during pregnancy are very common symptoms and are rarely due to a serious problem. Evidence suggests that 50% of women experience this pain during pregnancy. More than half of these women will complain that the pain impacts on their daily living. If you are starting to suffer from back or pelvic pain, make sure you are following all the advice and exercises previously listed on this page.Pain relief
If your back continues to be painful, there are a number of other things you can do to help yourself. For example:- Put an ice pack (bag of frozen peas wrapped in a damp towel) or hot water bottle on the painful area for 1–15 minutes, several times a day. Avoid placing it directly over your abdomen (tummy) and protect your skin with a towel.
- Relaxation and massage techniques can also help decrease the pain.
- Keep active, as staying still for prolonged amounts of time can cause joints to become stiff and painful.
- Talk to your pharmacist, GP or midwife about suitable pain relief to use during pregnancy.
- You may like to try this gentle stretch, which may help to relieve your lower back pain.
 Remember – it is not usually the one time we lift awkwardly or stand badly that causes pain; it is often the continual stresses and strains we place on our body during our everyday activities.
Therefore, it is important to modify your daily activities using the techniques in this booklet, do some of the gentle exercises we suggest and ensure you pace your activities throughout the day and week.
Please ask your midwife or GP to refer you to a physiotherapist if you are still having difficulties with pain.
Remember – it is not usually the one time we lift awkwardly or stand badly that causes pain; it is often the continual stresses and strains we place on our body during our everyday activities.
Therefore, it is important to modify your daily activities using the techniques in this booklet, do some of the gentle exercises we suggest and ensure you pace your activities throughout the day and week.
Please ask your midwife or GP to refer you to a physiotherapist if you are still having difficulties with pain.
How can I stay active?
Start by exercising the parts of your body most under strain during pregnancy. your back, tummy and pelvic floor muscles all need regular exercise to remain strong. Gentle low impact exercise, such as walking, swimming, yoga and pilates, is safe and highly recommended during pregnancy. Exercise encourages the release of hormones called ‘endorphins’ which help you to feel good, sleep better and reduce pain. However, there are some rules to exercise during pregnancy:- We advise that you avoid contact sports such as hockey/netball.
- Be sure you warm up and cool down to avoid injury.
- Make sure you do not get too breathless and can still talk in full sentences.
- Replace, reduce or stop high impact exercises such as running and jumping.
What is perineal massage and how can it help?
The perineum is the area between the vagina and the anus (back passage). Perineal massage is used to stretch the perineal tissue and scar tissue during late pregnancy. It may help to desensitise the area and reduce any pain. This may also help with a return to sexual relations.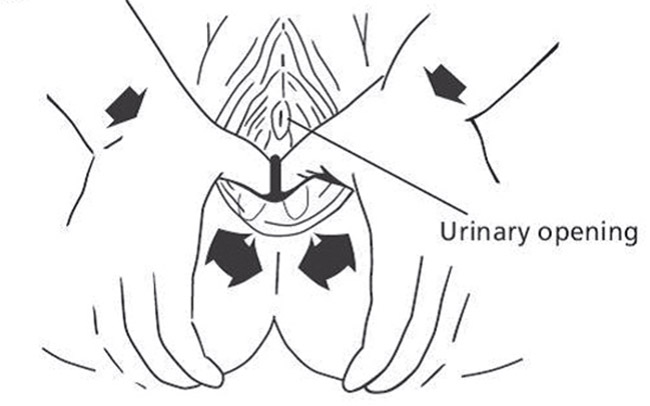
How to perform massage
Prepare
A mirror can help you to locate the area between the vagina and the anus so you know what you are doing. Imagine your perineum represents a clock face. Hands should be clean with nails clipped, Make sure your bladder is empty. Some women find having a warm bath beforehad can help relax and soften the tissue.Position
Position yourself so that you are comfortable. You could try:- Squatting down (supporting yourself by leaning back against a wall or forwards on a bed or chair).
- Sitting on the toilet
- Standing with one foot raised on a chair/toilet
- Leaning back or kneeling on all fours
Technique
Lubricate your fingers well using a vegetable oil (such as almond or olive oil). Insert one or two fingers up to 2 to 5 centimetres into the vagina. Massage the oil into the tissues of the perineum and inside the vagina. To prepare the tissues, start by pressing towards the anus and then use a firm sweeping movement down and to the back. Imagine your fingers are sweeping like clock hands from 3 to 9. Continue this for 2 minutes maintaining pressure throughout. Following this, apply a firm pressure at 5, 6 and 7 on the imaginary clock. Hold each stretch until you feel a burning, stinging sensation for approximately 2 minutes. This technique may be painful/cause stinging sensation – this is normal.
Try working in a circular montion with your thumb or fingertip across the scar and concentrate on one area of the scar at a time. Begin with a gentle pressure and build up as you feel comfortable.
Massage can also be performed in the bath without addition of any oils.
Following this, apply a firm pressure at 5, 6 and 7 on the imaginary clock. Hold each stretch until you feel a burning, stinging sensation for approximately 2 minutes. This technique may be painful/cause stinging sensation – this is normal.
Try working in a circular montion with your thumb or fingertip across the scar and concentrate on one area of the scar at a time. Begin with a gentle pressure and build up as you feel comfortable.
Massage can also be performed in the bath without addition of any oils.
Frequency
Aim to practice the techniques 3-4 times per week for between 5-10 minutes. Massage may be continued until the area is desensitised and less painful.Further information
NHS Choices – exercise in pregnancy Pelvic obstetric and gynaecological physiotherapyHelp and advice
If you have any concerns, or would like further advice, contact yoru local antenatal clinic, your community midwife or GP.Acknowledgement
This content has been produced by the Department of Women’s Health Physiotherapy, Imperial College Healthcare NHS Trust and is used with permission.Infections and viruses
Infections and viruses
Lifestyle information

Lifestyle information
Health and wellbeing in pregnancy

Health and wellbeing in pregnancy
Getting help

Getting help
It can be difficult to talk about how you are feeling and ask for help.
Common reasons for this are:
- you may not know what is wrong
- you may feel ashamed that you are not enjoying your baby or coping as you believe you should
- you may worry that your baby will be taken away.