This is a procedure in which a doctor, or specialist midwife attempts to the turn the baby into the correct position using gentle pressure on your abdomen with their hands.ECV is successful in about 50% of women and is generally safe. One in every 200 babies will need to be delivered by emergency caesarean after an ECV, and your baby will be monitored before and after the procedure to ensure they remain well.
Moxibustion for breech babies
This is a traditional Chinese technique which can be used to turn breech babies. It is done by burning a moxa-stick (a tightly packed tube of dried herbs) between the toes from 34-36 weeks of pregnancy. It has no known negative side effects and evidence suggests it can be successful at turning a breech baby (see here). You can ask your midwife or local acupuncturist for more information.
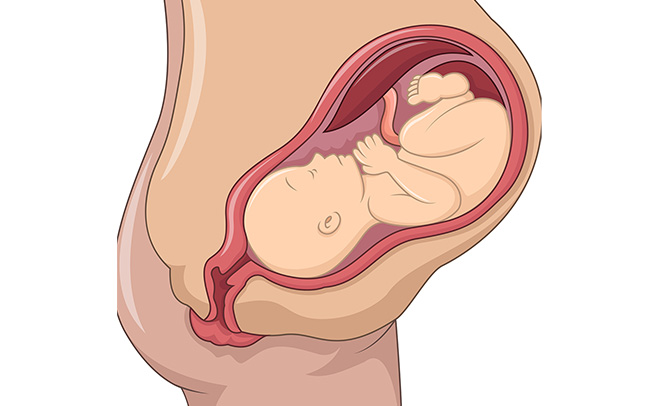
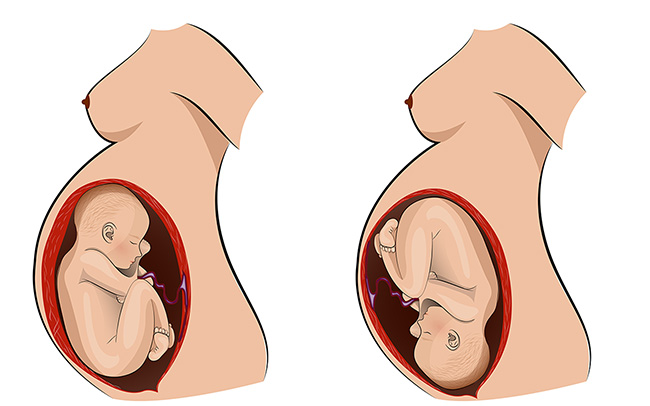
From 36 weeks pregnant, your baby should turn to the head down (cephalic) position in preparation for birth. A small number of babies will not be in this position, and may be either breech (bottom first) or transverse/oblique (lying sideways across your abdomen). If your midwife suspects that your baby is not in the head down position, you may be offered a scan and appointment with a doctor/specialist midwife to discuss your options. These options can include either attempting to turn your baby (see related links below), vaginal breech birth or planned caesarean birth.If your baby isn’t head down, don’t worry – there are many options available to you and your team will help you to make any decisions regarding your care moving forward.
When you choose to stop work is a matter of personal preference, but it is worth considering your commute, your working environment, your proximity to your maternity unit and allowing time to prepare for your baby’s arrival. You can discuss this with your midwife or doctor.Towards the end of pregnancy you may feel quite tired and uncomfortable, and therefore may need help from friends or family to get things done, particularly if you have other children. It’s important to stay active but to also make time for rest, particularly if you aren’t sleeping too well.
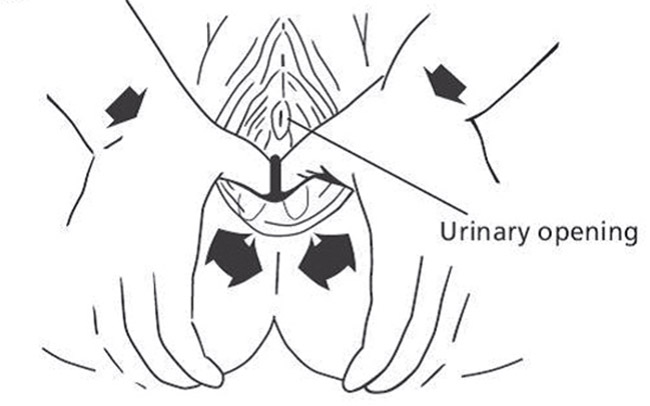
Massaging the perineum (the area between the vagina and anus) in the later weeks of pregnancy has been shown to reduce the likelihood of tearing during birth, and of needing stitches or an episiotomy. You can start this from when you are 34 weeks pregnant and practice it daily/every other day until the birth of your baby.How to massage your perineum:
wash your hands
sit comfortably with your legs bent at the knees so you can reach your perineum easily. Use a mirror if you wish
massage oil (preferably vegetable-based) into the skin of the perineum using fingers and thumbs
place one or both thumbs inside your vagina and press downwards towards the anus. Move to each side in a U-shaped stretching movement. This may give a tingling/burning sensation
aim to massage the area inside the vagina, not necessarily just the skin on the outside
Towards the end of pregnancy, you may feel a variety of different emotions as the birth becomes closer. You may feel excited, anxious or even scared – this is all normal. There are things that you can do to help you prepare for birth.
Completing a birth preferences plan can help you and your birth partner to think about your choices and preferences during labour and the birth of your baby. During your pregnancy you will have the opportunity to meet with your midwife/doctor and discuss the plan – try and do this around the time of your 34 or 36 week appointment. This will help your team understand the kind of birth you would like.Read the in app content about labour and birth, then using the birth preferences plan in the Personal care and support plans section write down your thoughts and preferences. See below for what options to consider.
how you feel about having a student present during labour/birth
different pain relief options for labour and birth
different positions for labour/birth
coping strategies and pain relief
how you feel about vaginal examinations
whether you would like continuous or intermittent monitoring of the baby’s heart during labour
any preferences you have if an assisted birth is recommended.
who will cut the cord/optimal cord clamping
skin-to-skin contact
your thoughts about infant feeding
how you would birth your placenta (afterbirth)
vitamin K for your baby.
It is useful to think about how you would like your baby’s birth to be in the event of having an induction of labour or a caesarean birth – planned or unplanned, and to ask your midwife or doctor what things you might need to consider for your own personal circumstances.Your midwife will discuss your preferences with you again when you are in labour and any reasons to consider changing the plan. You can share your birth plan with your midwife when you meet at the maternity unit (or at home if you are planning a homebirth).Complete your Personalised birth preferences plan in this app which can be printed out to share with your maternity team.
Would you like to talk with somebody about your options for place of birth?
Some women may find it helpful to talk to someone about their birth options. This is especially true if they have had a pregnancy, labour or birth that was difficult previously, or if something unexpected happened. It is not unusual to be unsure about your options or what effect any choices may have on this pregnancy and birth.You can speak to your midwife, and if needs be she will refer you to a birth options clinic, which is normally run by the consultant midwife at your chosen maternity unit.If you are considering requesting a planned caesarean birth, this decision would be made with you and the specialist midwifery and obstetric teams. Ask your midwife to refer you to the appropriate clinic, where you will be able to discuss your options.
Safety is always the priority, so if you have certain needs or complications with your health and/or pregnancy it may mean that giving birth on a labour ward is the safest option. Your midwife or doctor will discuss this with you if it is their recommendation.If this is your first baby, and your pregnancy is considered low-risk, it is just as safe to have your baby in a midwife-led birthing centre as it is to have your baby in a labour ward. Research shows the risk to the baby is slightly increased when planning to give birth at home.If this is your second or subsequent baby, it is just as safe to have your baby at home as it is to have your baby in a midwife-led unit or in a labour ward. Women who give birth at home, or in a midwife-led birthing centre are much less likely to require medical assistance including caesarean section, instrumental delivery, blood transfusion and episiotomy.
This is a decision you will make following discussion with your midwife or doctor at around 34-36 weeks of pregnancy, but it is helpful to start thinking about your preferences before this time.
Portal: Choosing place of birth
You can change your mind about where to have your baby at any point. If you choose to have your baby at home or in a midwifery led unit (birth centre), some events or complications before or during labour may mean transfer to the labour ward is advised.
Home
At home – in the comfort of your own home with the support of two midwives and whoever you choose to have with you. You can hire a birthing pool and your midwife can provide gas and air (entonox) if you want to use it.
Midwife-led unit (MLU)/ birth centre
This is a ward within the maternity unit. It is a homely and calm environment that supports normal birth with minimal assistance. Midwives and chosen birth partners are on hand to support you. You will have the choice of a birthing pool, gas and air (entonox), aromatherapy and opiate based pain relief, depending on your maternity unit of choice.
Obstetric-led unit (OLU)/ Labour ward/Delivery suite
This is a ward in a maternity unit where your care will be provided by a team of doctors and midwives. Normal birth with minimal intervention is always the goal, if it is safe to do so. Access to more specialised medical facilities and equipment is available for those women who need it.

 This is a procedure in which a doctor, or specialist midwife attempts to the turn the baby into the correct position using gentle pressure on your abdomen with their hands.
ECV is successful in about 50% of women and is generally safe. One in every 200 babies will need to be delivered by emergency caesarean after an ECV, and your baby will be monitored before and after the procedure to ensure they remain well.
This is a procedure in which a doctor, or specialist midwife attempts to the turn the baby into the correct position using gentle pressure on your abdomen with their hands.
ECV is successful in about 50% of women and is generally safe. One in every 200 babies will need to be delivered by emergency caesarean after an ECV, and your baby will be monitored before and after the procedure to ensure they remain well.