Exercise is an important aspect of a healthy lifestyle and generally the time you can resume exercise is a matter of personal choice. If you’ve had a caesarean it is important to wait at least eight weeks. Most women choose to wait until after their six week postnatal check with the GP before resuming exercise. When you start exercising it is important to remember to:
stop if it hurts
stop if you have any pelvic floor concerns, eg, if you notice any leakage of urine or experience a feeling of vaginal heaviness during exercise
stop when you are tired
never exercise when you are feeling unwell.
Try to avoid high impact exercise (jogging and jumping) for at least three months after birth. High impact exercise can put unnecessary strain on muscles, joints and the pelvic floor.Find out if there are any local postnatal exercise, yoga or Pilates classes near you. This can help with motivation and provide a social outlet.Remember that each woman’s recovery after birth is different, and avoid comparing yourself to others or setting unrealistic goals. Trying to incorporate gentle exercise into your daily activities is a great start, and it’s important to have plenty of rest as well.
After you have had a baby it is important to wait until you and your partner feel happy, ready and comfortable before resuming sexual intercourse. The timing of this will be individual to each couple. Some factors may increase the time you choose to wait before having intercourse. If the birth has been traumatic, physically or mentally, it may take longer for you to feel ready to have intercourse.
Some women have reduced interest in intercourse following childbirth, particularly if breastfeeding. More often than not your libido will slowly return to what was normal for you. A lasting low libido can be a sign of postnatal depression or post-birth trauma. It can help to talk to your partner, midwife, friends, family, health visitor, or GP to see what help and support might be available.
Many women find that sex is painful after birth, and that they are less lubricated naturally than they were before. Using a lubricant can help, as can taking
it gently and communicating with your partner. If sex continues to be painful, you can
always seek support from your healthcare provider. Intimacy can take on many forms and
does not necessarily need to include penetrative vaginal intercourse. Kissing,
foreplay, cuddling, mutual masturbation, oral sex and other forms of intimate play can
be less pressured whilst helping you to connect with your partner.It is possible to become pregnant again from just three weeks after the birth even if you have not had a period and are breastfeeding, therefore it is important to consider using contraception to avoid an unplanned pregnancy. Research suggests that becoming pregnant again within 12 months of having a baby can increase the chance of your baby being small for gestation, premature or even stillborn.Some maternity units are able to supply contraception before you are discharged home from the hospital. Your midwife will discuss your options during your pregnancy as it is easier to think about these before the arrival of your baby. Babies can be time-consuming and it may be difficult to access reliable contraception once you are home. All of the methods listed below are safe whilst breastfeeding. Ask your midwife for information on what is currently available in your maternity unit.Intrauterine contraception can be inserted at a planned (elective) caesarean section. A device (coil) is inserted into your uterus after birth and can remain there providing reliable contraception for 5 to 10 years, depending on the type (hormonal or non-hormonal).An implant, which is a matchstick sized rod inserted under the skin of your upper arm, can also befitted before discharge. The implant slowly releases progestogen hormone and provides reliable contraception for 3 years. The benefit of these methods which are known as long acting reversible contraception (LARC) is that you don’t need to remember to use contraception every day and therefore they have very low failure rates. Both intrauterine contraception and implants can be removed at any time at your GP Practice or local Family Planning/Sexual Health Services.Alternatively, a six month supply of progestogen-only pills or a progestogen-only injection which provides contraception for 13 weeks can be made. The failure rates of both these methods are much higher if they are not taken exactly as recommended, for example if you forget to take pills or do not receive your next injection when it is due. Your GP practice or local Family Planning or Sexual Health Clinic can provide you with further supplies of these methods.Ask your midwife about the advantages and disadvantages of each method to help you decide which method might be suitable for you.Find further information here:Contraceptive choices after you’ve had a baby
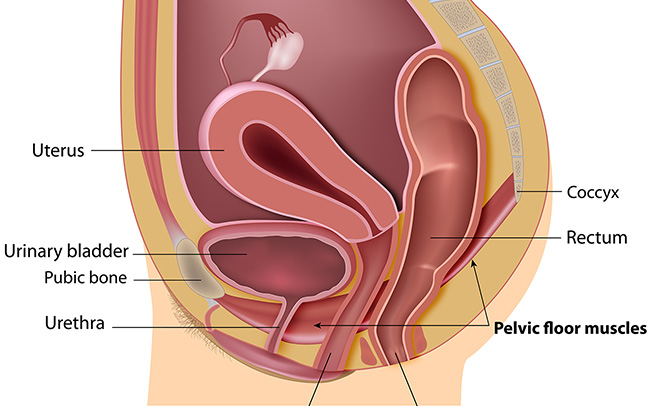
The pelvic floor muscles support your pelvic organs, stabilise the pelvic joints and are responsible for the control of bladder and bowel functions. These muscles are stretched during pregnancy and birth – which can sometimes lead to weakness or dysfunction during pregnancy and particularly after birth.Strengthening these muscles will:
maintain or improve bladder and bowel control
reduce the risk of prolapse of the pelvic organs
help to stabilise the joints of the pelvis and lower spine.
Exercises should be started as soon as your catheter (if you have had one) is removed and you have passed urine. The exercises can help reduce swelling and pain as well as treat/prevent incontinence. They should be completed at least three times a day. It can take up to three months for the muscles to regain their strength.
How to do your pelvic floor exercises
Lay or sit down comfortably and begin by imagining you are trying to stop yourself from passing wind/urine by squeezing the muscles around the back passage and vagina. Don’t do this whilst on the toilet, and don’t hold your urine as this can lead to problems with bladder function. You should work this muscle in two ways:
Hold the squeeze for a few seconds and then relax. Repeat this up to 10 times, gradually holding the squeeze for longer (up to 10 seconds).
Squeeze and release straight away. Repeat this 10 times.
Period type pains after the birth of your baby are normal and are caused by the contraction of your uterus as it returns to its pre-pregnancy size and tone. It is normal for these pains to feel stronger when you breastfeed your baby due to the effect of hormones released during a feed, causing the uterus to contract. Any severe after pains can be treated with paracetamol. Make sure you read the label, and speak to your local Pharmacist if you are unsure about this medication.If you are experiencing any symptoms of infection with your after pains see Feeling unwell.
The milk that your breasts first produce is called colostrum, and this will be present in the breast from mid-way through your pregnancy. Colostrum helps protect your baby from allergies and disease. Colostrum is concentrated breastmilk that comes in tiny amounts which is sufficient for the baby for the first three days.Around three days after birth, the colostrum changes and becomes mature milk – and this change may make your breasts feel heavy and tender. Engorgement is common and can happen when your milk “comes in” or if your breasts become over full of milk, especially when your baby is not latched on to the breast effectively. Engorgement can be relieved with frequent breastfeeding. If your breasts feel so full that your baby is unable to take the breast, try hand expressing a little of your milk before attempting to latch baby to the breast. See How to hand express.If your breasts are not relieved by feeding and hand expressing, seek help urgently. See Help with breastfeeding.Engorged breasts can progress to mastitis rapidly. Mastitis is an infection that can occur when milk ducts become blocked. Additional symptoms include a high temperature, and or lumps in your breasts that are hot, red and painful.
If you are experiencing symptoms of mastitis contact your midwife, GP or the maternity triage/assessment centre where you give birth urgently.
It is not uncommon to experience backache after the birth, particularly if you have had an epidural in labour. This is completely normal and should resolve in time with rest, warms baths and mild analgesia. If pain continues, speak to your midwife or doctor.See the POGP Fit for Future booklet in the related link for tips on how to manage back pain after birth.
Many ladies are anxious about opening their bowels for the first time after delivery, especially if they have had stitches. It is important that you try not to put off opening your bowels once you have had the urge to go, as this can make you more constipated.If you have been prescribed laxatives please use these as you will need to ensure that your stols remain soft but not watery. It is important to keep your stools like a ‘toothpaste’ consistency.To help prevent constipation you will need to maintain a good fluid update (2.5 – 3 litres if breastfeeding) and a healthy diet rich in fibre.Make sure you sit in a good position on the toilet to ensure you completely empty your bowels. The ideal position is:
knees higher than your hips (to do this place your feet on a step or point your toes)
lean forward and put yuor elbows on your knees
bulge your abdomen outwards as you take a breath in and straighen your spine
if you have discomfort, or are worried about the stitches you can hold a sanitary pad or a wad of tissues with your hand and apply pressure to the vagina and perineum
Piles (haemorrhoids)
Piles are swellings of the blood vessels inside or around the rectum, and are very common following pregnancy and birth. In most cases, piles will disappear without treatment within a few weeks of birth. Ask your midwife, doctor or local pharmacist for advice regarding piles if you think you may have them, or if they become painful.
After delivery, your midwife will give you a bowl to measure your urine in. It is important for your midwife to know the volume of urine to ensure your bladder is working properly.You may have a catheter post-delivery. After the catheter is removed it is important that you pass urine within six hours. If you don’t, you must tell your midwife or doctor immediately.If you are having difficulty passing urine or have not had an urge to pass urine four hours after your catheter has been removed try:
going to sit on the toilet, relaxing and leaning forwards
turning on the taps so you can hear running water or pulling lightly on the pubic hair (both of these can help to stimulate an urge)
rocking forwards and backwards on the toilet
gently tapping over the bladder near your pubic bone for a few minutes
After birth, some women find that their bladder function is not as efficient and can experience:
urinary retention (when the urge to pass urine is absent or isn’t as strong – this leads to the bladder overfilling. This over-stretching can cause long-term damage to the bladder)
stress urinary incontinence (when urine leaks on sneezing, coughing or exercising)
urgency urinary incontinence (when you suddenly need to pass urine with no prior sensation to do so – leading to leaking of urine).
Pelvic floor exercises can help improve bladder function, however if you are worried about your urinary control, or any symptoms of bladder dysfunction persist it’s important to speak to your midwife, health visitor or GP.
Some bleeding after birth is normal – this is recorded in your notes as estimated blood loss (EBL). Vaginal bleeding after birth is referred to as lochia, which is a mix of blood and other products from inside the uterus. This can be quite heavy at first, requiring several sanitary pad changes a day. After the first week the lochia slows down and becomes pink/light brown in colour. This loss will normally disappear by four weeks after birth.Any large clots, silky membranes, sudden heavy bleeding or an offensive smell may be a sign that something is wrong and should be discussed with your midwife or GP urgently.
Retained products
You may be aware that when the placenta detaches from the inside of the uterus sometimes small pieces or fragments are left behind. Your midwife will have checked the appearance of the placenta to check whether there are any obvious pieces missing, but it is not always possible to spot fragments that have been left behind. The same is true when a caesarean is performed. Even though the doctors will have checked the inside of the uterus for any remaining placenta, it is not always possible to identify them.For most women, any retained fragments of placenta (sometimes referred to as “retained products”) will pass unnoticed with the normal lochia in the days or weeks following the birth. However, for a small number of women, retained products that do not pass naturally may require medical assistance. It may be that heavy bleeding occurs, or you begin passing blood clots. Or you may develop a temperature and feel shivery and unwell. These are potential signs of retained products that require treatment and if you develop any of these symptoms, you should get in touch with your local maternity Triage, or see your GP.Occasionally the retained products require surgical removal. This will involve a short procedure under a general anaesthetic, but most women can go home the same day.

 Exercise is an important aspect of a healthy lifestyle and generally the time you can resume exercise is a matter of personal choice. If you’ve had a caesarean it is important to wait at least eight weeks. Most women choose to wait until after their six week postnatal check with the GP before resuming exercise.
When you start exercising it is important to remember to:
Exercise is an important aspect of a healthy lifestyle and generally the time you can resume exercise is a matter of personal choice. If you’ve had a caesarean it is important to wait at least eight weeks. Most women choose to wait until after their six week postnatal check with the GP before resuming exercise.
When you start exercising it is important to remember to: